Most of the parts of this theory of ME/CFS etiology are not novel, but I think this ultra specific arrangement of them is. So, I will give credit where credit is due: @Hip on the forum phoenixirising, Jen Brea, Jeff Wood (@jeff_says_that on twitter), the author of the site that started all of this structural me/cfs interest, and Erik Johnson (@erikmoldwarrior) for coming up with a) the idea that mold was a major issue in me/cfs, and for going further and theorizing that nanoparticles combined with mold spores would make them more pathogenic.
I will also try and make the organization chronological, from embryo to adult.
And I will try and break down pathology from macro to micro levels in a way that makes sense, and include a summary of both the theory and the important gaps left to fill/investigate, at the end.
In utero:
- Neural tube defects, either congenital tethered cord or chiari, are likely to be an issue in me/Cfs patients, and can be caused by in utero exposures to organophosphate pesticides like chlorpyrifos.https://www.sciencedirect.com/science/article/pii/S2090506815001049 , https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6029725/
- Often these issues are only mildly symptomatic until a major infection or environmental exposure
- Some sort of hyper mobile phenotype
- Again not necessarily symptomatic, and perhaps not fully meeting criteria for a connective tissue disorder, but some level of hyper mobility, seems somewhat common in this population
Onset/Trigger of ME/CFS
- Infection
- Certainly the most common reported trigger https://www.cdc.gov/me-cfs/about/possible-causes.html
- Probably not sufficient to cause me/cfs on it’s own, eg we dont know why the ~10 percent of patients with mono or ~25 percent of patients with Lyme disease go on to develop a chronic illness while the rest fully recover
- Everything from sars 1, to covid-19, to enteroviruses, to h1n1, has similarly triggered ME/CFS
- Environmental exposure
- Most commonly reported is mold exposure. However pesticide exposures and other chemicals are plausible too.
- Very specific outdoor toxins/bio toxins have been reported to be associated with me/cfs, not just moldy buildings, but these have not been identified and studied, so most of what I say here is theory and speculation. As a side note, I personally think that the indoor and outdoor toxins are the most important triggering and maintaining factor in this illness. We dont know exactly what these toxins or combinations of toxins are, but we have guesses and theories, some that are backed up by recent scientific literature (nanoparticle theory) https://paradigmchange.me/wp/outdoor-toxins/ https://www.pnas.org/content/115/27/7087 https://cfsuntied.net/2014/12/04/and-now-for-something-completely-different/
- Heavy metals–either through ingestion or nanoparticle inhalation (car exhaust is a common form of this), or through fog (mercury fog https://news.ucsc.edu/2019/11/wilmers-mercury.html )
- Or, Dual Factor theory
- A combination of immune suppressant and an infection. The immune suppressant can be an environmental exposure , although not limited to https://forums.phoenixrising.me/threads/me-is-not-mould-intolerance-mould-intolerance-is-not-me.51792/page-6#post-856637
- Cite studies on immune suppressing effects of various bio toxins, and also the fungal/viral colonization together making things difficult for immune system trichothecenes immune suppression , zinc nanoparticles increase cyanobacteria toxicity/immune suppression
- “I always found it very perplexing that infectious epidemic outbreaks of ME/CFS could cause such severe disease, and yet not spread much further than the localized environment, apart from perhaps some sporadic appearing as the virus spreads outwards. To me, that makes it impossible that epidemic ME/CFS is caused by a virus alone, because if it were just a virus, then that virus would have spread to the whole region or country, and caused the same devastation throughout.
But it seems that as these viruses leave the vicinity of these outbreaks, they lose most of their ability to cause ME/CFS.
To my mind, that means there must have been some local cofactor (such as a toxin) present only in the vicinity of the outbreak — a cofactor which in combination with the virus then causes ME/CFS. And as soon as the virus spreads further than the local area containing the toxic cofactor, the virus loses most of its ability to trigger ME/CFS.”–@Hip
- Physical trauma
- Car accidents, whiplash etc
Central pathologies (post trigger)
- Macro
- Ligament damage from post infectious/toxin exposure induced inflammation, combined with congenital tethered cord, leads to craniocervical instability. The cervical instability leads to brainstem compression. https://medium.com/@jenbrea/onset-part-ii-mold-damage-9f9b37cf5a80
- Csf flow is blocked either by chiari or cci, causing high intracranial pressure. Csf flow blockage also leads to impairment of brain detoxification, especially during sleep The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions
- Brainstem compression from cci
- Causes global hypoperfusion?
- Causes hypometabolism?
- Causes inflammation both directly (by injury activating glia) and indirectly (by causing impaired detoxification, blocking csf flow, and causing an inflammatory response to the toxins the body hasn’t dealt with)
- Causes autonomic issues, pots, OI, apnea of various kinds, hypoxia, gut motility issues
- Causes PEM as a result of impaired blood flow/autonomic function?
- Causes gaba/glutamate imbalance
- Causes headaches/coat hanger pain
- summary of all of the above here
- Chiari
- Similar to cci–both cause cervicomedullary syndrome and csf flow blockages
- Tethered spinal cord
- Causes hypoperfusion of spinal cord
- Causes bladder issues
- Causes fatigue
- Causes hypometabolism
- Causes PEM, impaired oxygen extraction from muscles
- https://medium.com/@jenbrea/pathology-part-ii-could-pem-be-a-symptom-of-neural-strain-f5be69175e1
- Micro (cellular level/molecular)
- Inhaled toxins/pollutants/irritants lead to brainstem inflammation. This explains the subset of people without cci who nevertheless are similar in severity and symptoms to cci patients. https://www.pnas.org/content/115/27/7087 , https://www.sciencedirect.com/science/article/pii/S1748013218306364 , https://www.frontiersin.org/articles/10.3389/fneur.2018.01033/full (last study showing brainstem inflammation in me/cfs patients as well as commenting on and critiquing methodology of brainstem imaging)
- Hypometabolism as a protective response to oxidative stress? Is this incompatible with mechanical issues causing hypometabolism? Dont think so, Naviaux has mentioned CCI as something that could cause the cell danger response, which is coordinated through pathways in the brainstem
- Specifically, as a result of brainstem compression/neural stretch injury, glial activation and whatnot.
- The problems in metabolism are not a primary issue and not solvable through thyroid hormone or supplementing any cofactors of the Krebs cycle. They are adaptive. https://www.pnas.org/content/113/37/E5472
- Inflammation from the innate immune response to novel toxins/pollutants, in the absence of a robust adaptive immune response. Allergies are adaptive
- High brain glutamate/lactate –due to physical trauma OR bio toxins (like domoic acid! Or penitrem a): https://www.sciencedirect.com/science/article/abs/pii/030439409190792R
Fun bonus? Glutamate receptors in the brainstem mediate sound sensitivity. Actually it’s not so fun. For me, as a former musician, sound sensitivity has been the worst part of my ME/CFS. Interesting to learn indirectly that both toxic exposure and brainstem injury could contribute to sound sensitivity.
In conclusion: a simplified model:
Someone born with tethered cord (not necessary but it helps) , gets an infection while living in an environment with toxins. Becomes one of the substantial minority of the people with that infection who have a chronic illness. The infection and environmental exposure lead to inflammation in the brainstem and globally, which in some patients damages ligaments, leading to craniocervical instability. So most or all patients end up with either inflammation in the brainstem or mechanical compression of this. This leads to very severe ME, the brainstem compression in turn blocks csf flow, which prevents the brain from proper detoxification, especially during sleep. Brainstem compression , cord stretching , and inflammation cause all or most of the autonomic issues, blood flow problems, and PEM in this illness. Csf flow blockage causes a vicious cycle in which the brain cannot properly detoxify, and thus the environmental toxins which caused the initial inflammation become even more of an issue, causing an inflammatory response while trying to expel them.
https://qz.com/689806/a-controversial-theory-may-explain-the-real-reason-humans-have-allergies/
And one last thought: I believe that despite the role of other things, such as infection and trauma, in this disease, the role of as of yet unknown environmental toxins/pollutants is very underrated. Connective tissue damage as a sequelae of infection is not unheard of, but , we don’t have good epidemiological data on how frequent these conditions are, and I believe them to be increasing. The environmentally caused inflammation may be the main difference separating those who have me/cfs post infection and those who dont. I would have high confidence in the ability to make an animal model of me/cfs based on these factors, if only we knew what the unknown environmental toxin was. That variable, agent x, needs to be found. Otherwise we will know how to treat ME/CFS but not cure it or prevent relapse.
My most plausible idea of what agent x is, is some kind of slurry of mold spores or mycotoxins, stuck to nanoparticles that are ubiquitously floating around as a result of industrial production of various sorts. But honestly, scientists should just be starting with the idea that we know nothing, except that there’s something in the environment causing this illness, and go hunting with air samples and mass spectrometers or NMRs. Is it that simple? I’m not a scientist so I’ve probably got some of this wrong. But I do know that this is a plausible theory that explains a lot of the evidence , both anecdotal and published literature, and presents testable animal models. And its parsimonious enough, especially considering the incredible complexity of ecological changes in the past couple of centuries.
One final footnote: craniocervical instability and tethered cord feature heavily in this hypothesis, so here are some links to learn more about them:
- https://onlinelibrary.wiley.com/doi/full/10.1002/ajmg.c.31549
- https://youtu.be/zpSXSMPiMI8
- https://www.mechanicalbasis.org/
- https://cfsuntied.net/2014/12/04/and-now-for-something-completely-different/
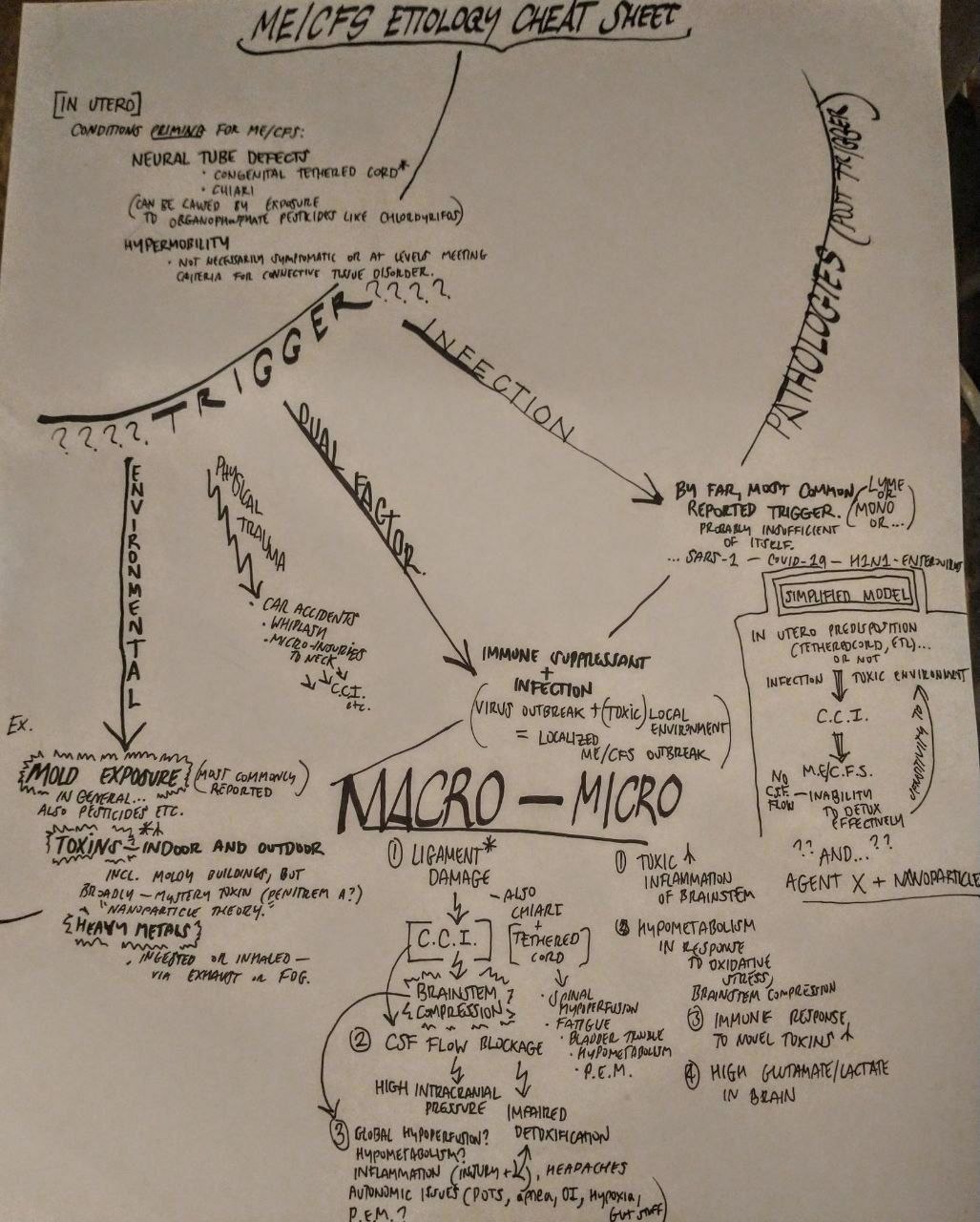
A drawn diagram trying to make sense of this complex etiological theory of ME/CFS–thanks to Theodore Naylor for drawing this
(Tags: nanoparticles, mold, mcas, cci, craniocervical instability, nanoparticles mold, nanoparticle fungal, nanoparticles, environmental causes me/cfs, nanoparticle, walker storz, nanoparticle, nanoparticles mast cell activation, robert naviaux, erik johnson, Jen Brea)
If you have any thoughts on this research, please contact tastorz@yahoo.com, wstorz@yahoo.com, or sammystorz@gmail.com. Thank you very much. I welcome criticism, or attempts to fill in the gaps of this theory.